

Dr Euan Mackinnon explores if we can achieve surgical outcomes using a non-surgical approach
Advances in dermal filler properties and handling means we can achieve pleasing results for many of our patients with relatively small volumes of product. However, sometimes small volumes simply will not be able to produce the desired results that patient and practitioner may be wishing to achieve. In these cases, a frank and honest consultation with patients is required to avoid disappointment. I have long been fascinated by large volume treatment plans and in essence trying to effect surgical results for my patients using non-surgical modalities.
In this case I will discuss my approach to a pan-facial treatment of a 30-year-old male using the Merz portfolio of dermal fillers. These fillers are my perfect armamentarium for pan-facial treatments. There truly is a product for every purpose that I require for my diverse range of patients. Naturally, when I inject higher volumes of products, I assume a higher level of risk both intra-operatively and post-procedurally. Therefore, it is imperative that I feel confident in the safety profile of my chosen injectables. I choose BELOTERO as it has demonstrated a lower risk of inflammation compared to some other leading HA fillers whilst delivering exceptional results.4 Due to its ‘Cohesive Poly-densified Matrix (CPM)’ technology, it offers the most homogeneous biointegration compared to other HA fillers and it really is a joy for me to inject due to its flowing qualities.4
The range allows for exceptional three-dimensional tissue expansion whilst maintaining natural facial appearances both at rest and on animation.
Patient concerns
Primary Concern: Retrognathic (retruded) mandible.
Secondary Concerns: Tired appearance when not feeling tired. Flattening of the midface. Does not want to look overdone.
Treatment desires
To have a stronger chin and jawline. To look more rested. To look more attractive.
Objective
Upper Third – Temple hollowing. No static upper face lines.
Middle Third – Deplete medial cheek fat pads with early evidence of malar split. Limited anterior cheek projection in profile. Limited zygomatic arch projection. Mild tear trough deformity.
Lower Third – Class 2 skeletal base. Retrognathic (retruded) mandible and overjet of upper incisors. Poor definition of mandibular body and angle. Long philtrum, narrow horizontal dimension of upper lip and scope to balance vertical proportions of both lips.
Surgical options
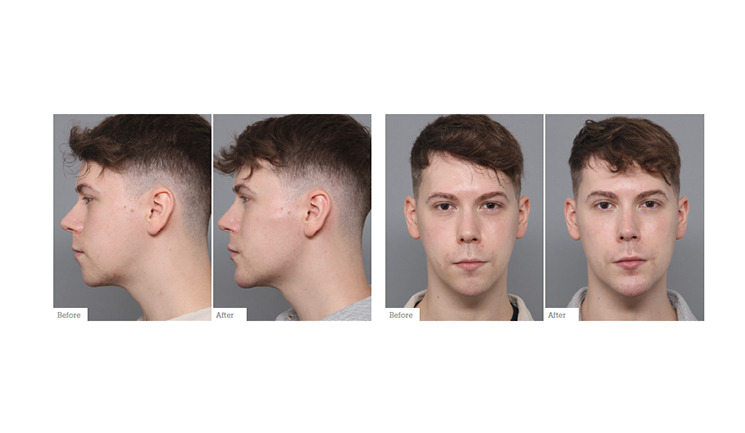
This patient certainly could be treated with surgery in a combined maxillofacial and orthodontic approach to correct his skeletal discrepancies. This may include a Le Fort 1 maxillary osteotomy, bilateral sagittal split mandibular osteotomy +/- sliding genioplasty. Facial fat transfer or customised implants may also be considered. However, this would come at the price of extensive orthodontic treatment, surgical risks, and prolonged recovery time. In this case we decided to use dermal fillers to mimic the effects of surgery. 16.5ml of dermal filler was injected during one treatment session. Post-procedural pictures were taken at two weeks.
The exceptional integration of the Merz products into the tissues enables the patient to express and emote in a completely natural manner
Treatment
Scan the QR code to watch me perform this pan-facial treatment

Temples: 2ml total. 1ml of BELOTERO Volume1 per side using a supra-periosteal technique over two injection sites. Care is taken to identify the superficial temporal artery prior to injection.
Cheeks: 2ml total. BELOTERO Volume.1 Cannula entry point at the zygomatic prominence. Product fanned sub-SMAS into the deep cheek fat compartments indirectly providing support to the SOOF. Cannula flipped posteriorly through the same insertion point along the inferior aspect of the zygomatic arch to produce a masculine cheekbone vector. N.B. for female patients, follow the superior aspect of the arch towards the temple.
Chin: 4ml total. BELOTERO Volume.1 Dual-plane technique. First, bone is simulated with supra-periosteal bolus placement to achieve better anterior projection and width. Secondly, a cannula is used sub-dermally to further enhance the anterior projection.
Jawline: 7.5ml total of RADIESSE.2 I use two cannula entry points for a full jawline augmentation allowing me to reach from the chin to the mandibular ramus. The more distal entry point allows posterior augmentation of the angle and ramus. The more proximal entry point allows augmentation of the mandibular body, pre-jowl region and inferior aspect of the chin.
My preferred jawline product for men is RADIESSE.2 I primarily use this in the subdermal plane. The product is stiff on injection but can be easily moulded. The Calcium Hydroxyapatite technology is biostimulatory and produces robust and long-lasting definition through neocollagenesis. Clinicians need to be mindful of the short-lived (1-3 days) inflammatory response that occurs after injection of RADIESSE2 and patients should be reassured and counselled on this pre-procedurally. This product is not hyaluronic acid based and should only be used by experienced injectors.
Lips: 1ml total. BELOTERO Balance.3 Sub-vermillion placement of product is my preference for men to allow for enhanced definition without creating an unnatural ledge at the lip border. The tubercles were then enhanced based on clinical experience with superficial injection of Belotero, no Tyndall effect has been observed.4

Summary
16.5ml of Merz Aesthetics dermal fillers were strategically injected in one treatment session. At two weeks there was full resolution of any minor post-procedural swelling or bruising, which is expected during a pan-facial treatment.
Although there will always be a place for operative facial procedures, the exceptional advances in non-surgical alternatives can now mimic surgical outcomes without the surgical downtime and risk. Other benefits include the potential for a staged treatment approach and reversibility of HA products. Drawbacks of non-surgical options include the need for repeat treatments at intervals and the associated accumulative cost to the patients over time.
This patient’s primary concern was his retrognathic mandible which has now been adequately corrected. He appears more rested with a more masculine appearance. He has more three-dimensional structure to his face without appearing over-filled. The exceptional integration of the Merz products into the tissues enables the patient to express and emote in a completely natural manner and he was thrilled with his results on review.
