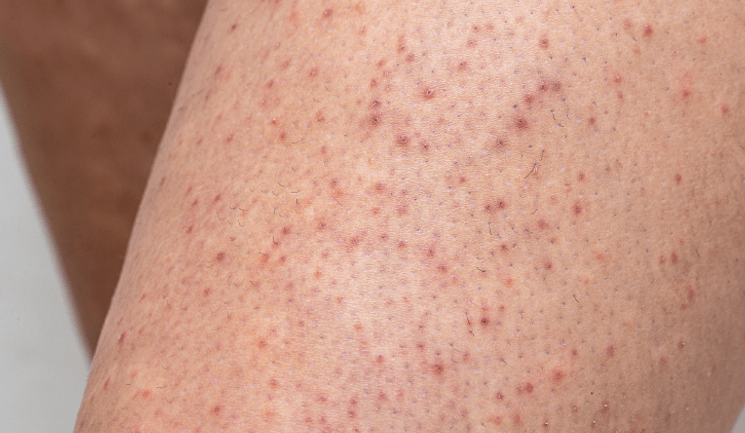
Different Treatment Options for Keratosis Pilaris




The UK’s leading monthly publication for medical aesthetic professionals.
The UK’s leading monthly publication for medical aesthetic professionals.
Kate Byng-Hall
on
May 11, 2023

0203 096 1228
2nd Floor, Regal House, 70 London Road
Twickenham TW1 3QS, United Kingdom
© 2023 Easyfairs UK Ltd | Registered in England No. 05067979